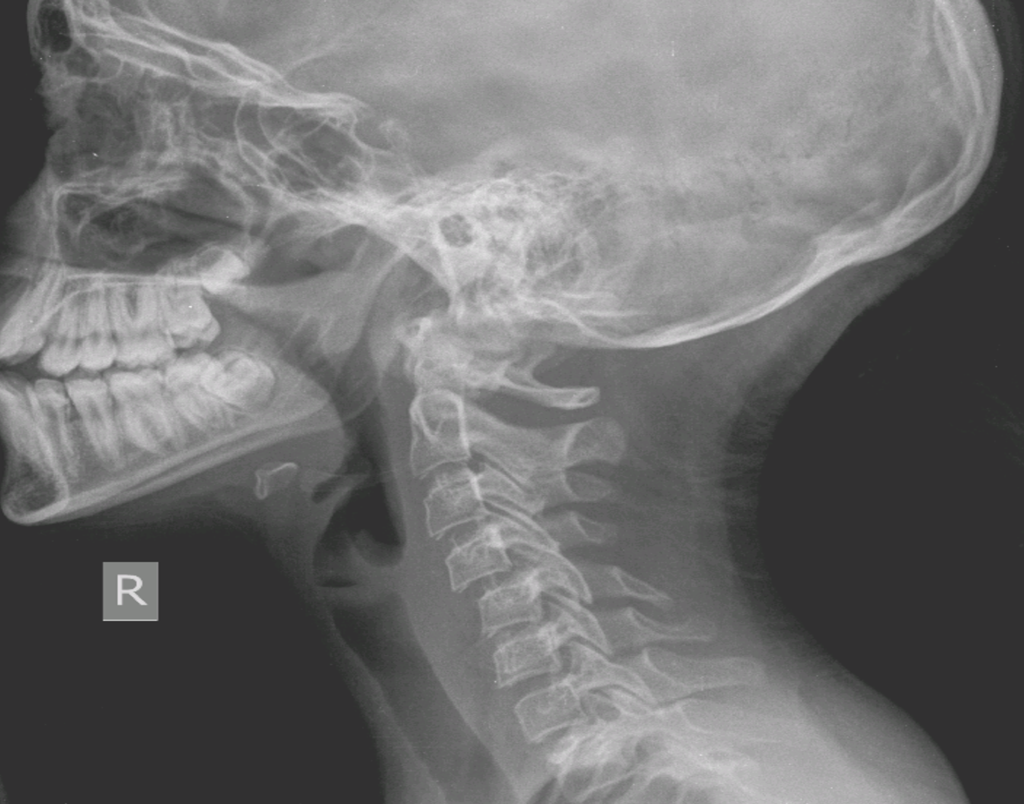
10 y.o. girl. Sport accident. Neck pain
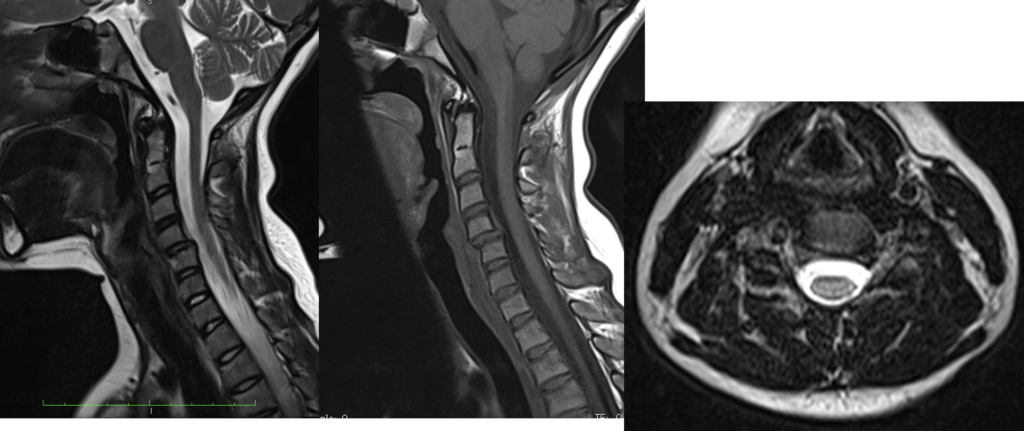
No neurology.
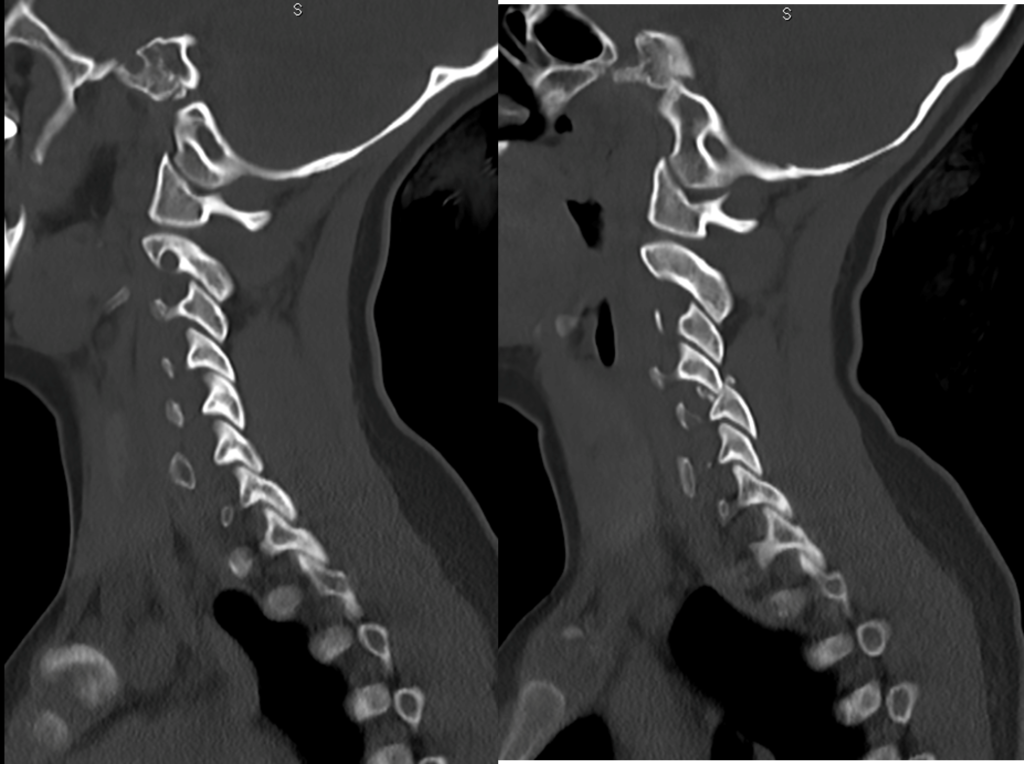
In may opinion, it is not necessary to restore the spine alignment with cervical traction. Alignment can be provided by posterior surgery. If superior part of inferior articular processes are removed bilaterally during the surgery, It is easy to restore the alignment by pulling down the C4 spinous process, the lateral masses can be brought closer together. In this way, both sides can be fixed by screwing in the lateral masses at the same time.
Ali Fahir Özer
C4-5 ACDF. Its a uni-facetal subluxation.
Arvind G Kulkarni
Thank you very much for sharing this case I think intra operative manual traction + ACDF will be satisfactory
Sameh Habib
Thank you for the nice case. In case of bilateral facet dislocation, mild traction and posterior release with lateral mass fixation could solve the problem of realignment and instability. However, unilateral facet dislocation may be reduced through ACDF with Casper vertebral distraction. This would also realign the segment and stabilize it. The only concern to me is the young age of the patient with high risk of adjacent segment disease later on. However, casualty surgeries are usually life saving and obligatory in many cases.
Mohamed Mohi Eldin
I think it’s a perched (jumping) facet ; not yet locked ; unilateral. Subluxation is less than 50%
I’d do closed traction in flexion under GA and neuromonitor followed by ACDF C4,5 especially if this incident is recent “reducible”. It would be more doable to restore alignment in pediatrics anteriorly due to soft tissue laxity.
I think chronic injury / bilateral locked facets > 50% subluxation / adults are more likely to need facet drilling posteriorly with lateral mass instrumentation after failure of closed reduction by traction trial in supine.
A. Bayoumi
This is a typical case of unilateral facet dislocation. I can’t see a difference between jumped facet and locked facet. But we know well if facet is fractures, reduction is easier. Flexion and rotation together are the mechanism causing such an injury. Since it is an acute case, anterior reduction will be easy and effective. Single level discectomy plus plating is my suggestion. I would not try closed reduction, it is a waste of time and even after closed reduction, you eed an open fixatiın.
Mehmet Zileli